Onset of axial spondyloarthritis (axSpA) begins before the age of 45, often occuring in the early 20s and 30s.
It affects men and women, with men generally experiencing a more progressive form of the disease.
Women typically experience a greater negative impact on their quality of life.
Go 6th slide
Introduction
Spondyloarthritis (SpA) refers to a group of heterogeneous conditions that share common pathologic and clinical manifestations.
Axial spondyloarthritis (axSpA) has a broad phenotype that includes:
Ankylosing spondylitis (AS), also known as radiographic axSpA, which is characterized by sacroiliac joint (SIJ) and spinal damage that may range from mild erosive disease to new bone formation and joint fusion.
Non-radiographic spectrum of disease (nr-axSpA), which occurs in those individuals who do not show any changes in the sacroiliac joints or the vertebrae on X-ray and may represent either early or mild forms of disease with the potential to progress into AS.
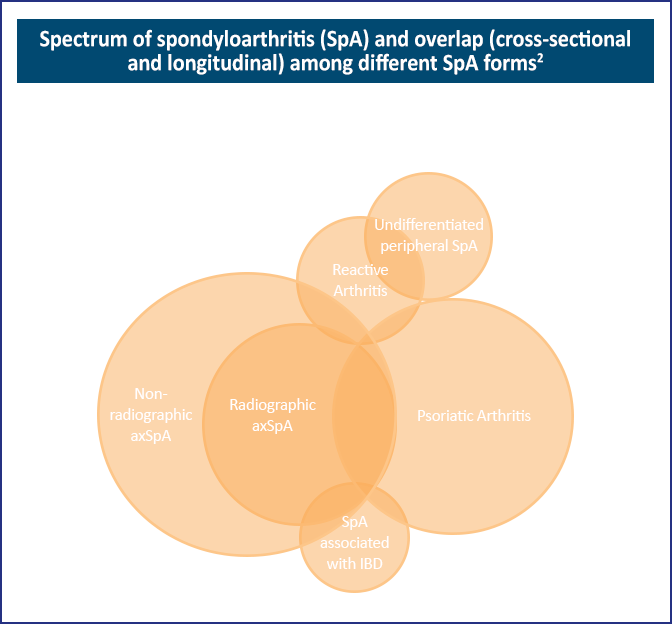
Other subgroups of SpA are largely characterized by peripheral joint involvement, eg, psoriatic arthritis (PsA), arthritis related to inflammatory bowel disease (IBD), and reactive arthritis. It is this diversity in clinical phenotype that has led to a divide between axial versus peripheral SpA. Clinical experience indicates that individuals with predominantly axial disease may develop peripheral joint involvement and vice versa, ie, individuals with typical peripheral SpA can develop axial involvement in an estimated 40% of cases.1
Figure: Spectrum of spondyloarthritis (SpA) and overlap (cross-sectional and longitudinal) among different SpA forms2
Recent research into the pathophysiologic mechanisms and immune substances that lead to chronic inflammation and pain has led to significant improvements in the care of patients with axSpA. In this Clinical Toolkit, you will find information about diagnostic criteria, recent treatment guidelines, and clinical trial data on current and investigational therapies that impact treatment selection. A list of additional references and resources is provided to help you improve the clinical outcomes of patients with axSpA.
Quality of life and patient burden
Symptoms of pain, stiffness, and fatigue associated with progressive bony fusion of the spine are major contributors to disease burden and limit physical functioning, including the ability to perform activities of daily living, such as dressing, walking, bathing, and eating.3 The physical limitations of axSpA can also affect employment, leisure activities, mood, and interpersonal relationships. Spinal deformation/curvature and poor posture can result in significant disturbances in body image, which are linked to higher rates of anxiety and depression.4 In addition, sexual dysfunction and dissatisfaction, impaired relationships with intimate partners, and lower urinary tract symptoms are significantly more common in men with axSpA than in matched control subjects.5 Emerging data show that axSpA tends to be associated with the development of certain comorbidities, including cardiovascular diseases, diabetes mellitus, osteoporosis, and depressive disorders.6
Roughly 66% of patients with axSpA experience fatigue, with sleep quality being a major contributor.3
Patients with axSpA report awakening 1.5 times per night, and 46% have moderate-to-severe insomnia.
In a study of men with axSpA, 45% switched to a less physically demanding job, and 24% retired early (mean age of 36 years) because of the condition.7
Epidemiology
AxSpA commonly starts in the second to third decade of life, with a male to female ratio of 2–3:1 for the radiographic form and 1:1 for nr-axSpA.8
The majority of epidemiological studies performed to date have been in AS, which has an estimated prevalence of 0.5–1%.1
The overall prevalence is variable, with estimates between 0.32% and 1.4%, depending upon geographical region and ethnicity.1
The prevalence of axSpA (0.9–4%) in the United States population is higher than the diagnostic prevalence (0.2–0.7%).9
The average age of symptom onset in axSpA is a bit later in women than in men; the lower prevalence of human leukocyte antigen (HLA)-B27 in women may account for the slightly longer diagnostic delay.1
The progression of patients with nr-axSpA to AS is slow, with estimates of 5.1% in 5 years and 19% in 10 years.10
While the risk of cardiovascular events and mortality is slightly increased in AS, no studies have examined these outcomes in the broader group of patients with axSpA.10
References
Dubash S, McGonagle D, Marzo-Ortega H. New advances in the understanding and treatment of axial spondyloarthritis: from chance to choice. Ther Adv Chronic Dis. 2018;9:77-87.
Proft F, Poddubnyy D. Ankylosing spondylitis and axial spondyloarthritis: recent insights and impact of new classification criteria. Ther Adv Musculoskelet Dis. 2018;10:129-139.
Shen B, Zhang A, Liu J, et al. Body image disturbance and quality of life in Chinese patients with ankylosing spondylitis. Psychol Psychother. 2014;87:324-337.
Dhakad U, Singh BP, Das SK, et al. Sexual dysfunctions and lower urinary tract symptoms in ankylosing spondylitis. Int J Rheum Dis. 2015;18:866-872.
Terenzi R, Monti S, Tesei G, Carli L. One year in review 2017: spondyloarthritis. Clin Exp Rheumatol. 2018;36:1-14.
Cakar E, Taskaynatan MA, Dincer U, et al. Work disability in ankylosing spondylitis: differences among working and work-disabled patients. Clin Rheumatol. 2009;28:1309-1314.
Sieper J, Poddubnyy D. Axial spondyloarthritis. Lancet. 2017;390:73-84.
Danve A, Deodhar A. Axial spondyloarthritis in the USA: diagnostic challenges and missed opportunities. Clin Rheumatol. 2019;38:625-634.
Wang R, Ward MM. Epidemiology of axial spondyloarthritis: an update. Curr Opin Rheumatol. 2018;30:137-143.