Early diagnosis of axSpA is crucial to minimize disease burden. Disease activity, patient-reported pain, and impairment to quality of life are high in the early stages of disease, independent of radiographic changes.4, 5 Underrecognition of axSpA results in a missed or late diagnosis, leading to prolonged pain, stiffness, fatigue, and decreased mobility.
Early treatment of nonradiographic and radiographic axSpA improves symptoms, function, and inflammation as viewed by magnetic resonance imaging (MRI) and may prevent irreversible changes.5, 6 If left unmanaged, chronic inflammation in the sacroiliac joint and spine over time can lead to pathologic bone formation, structural damage, and, ultimately, fusion of the sacroiliac joint and spine in some patients.2 This progression can lead to several clinical and quality of life challenges such as reduced range of motion, higher risk of fracture, spinal curvature, stiff rib cage, and even breathing restrictions.7
Longer delays in diagnosis are associated with greater radiographic progression, worse spinal mobility, less favorable response to treatment, reduced quality of life, and increased direct and indirect health costs.4, 5, 6
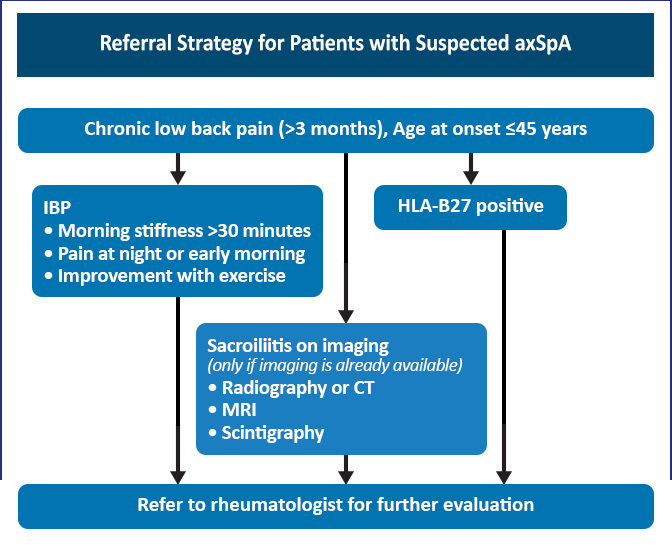
When axSpA is initially suspected, patients should be given a prescription for an NSAID as an interim first-line treatment while a rheumatology consult is arranged. Early initiation of physical therapy is also recommended. The decision to initiate biologic therapy should be deferred to a rheumatologist following confirmation of the diagnosis and assessment of the risks and benefits of therapy.2
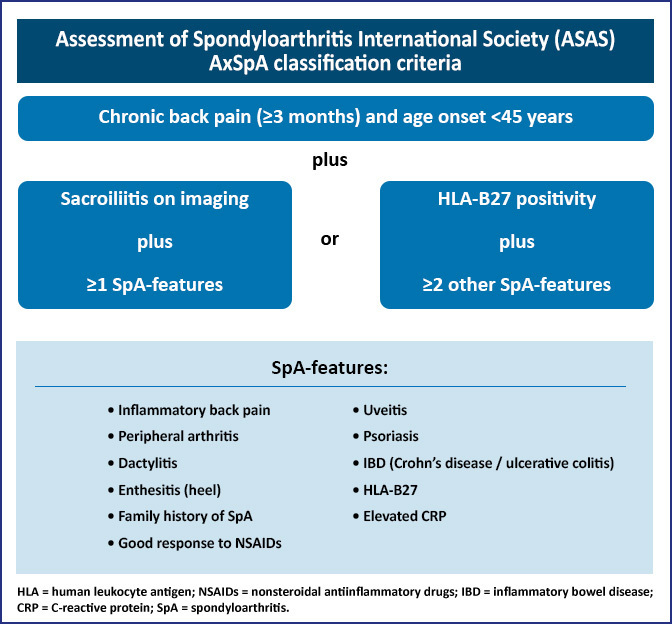
In general, the diagnosis of axSpA is a clinical judgment based on features that are characteristic of the disease. These features include a combination of historical manifestations, physical findings, laboratory results, and imaging data. Patients with suspected axSpA must be assessed carefully. Figure 3 lists the classification, but not diagnostic, criteria of axSpA.4
Figure 3: AxSpA Classification Criteria8, 9